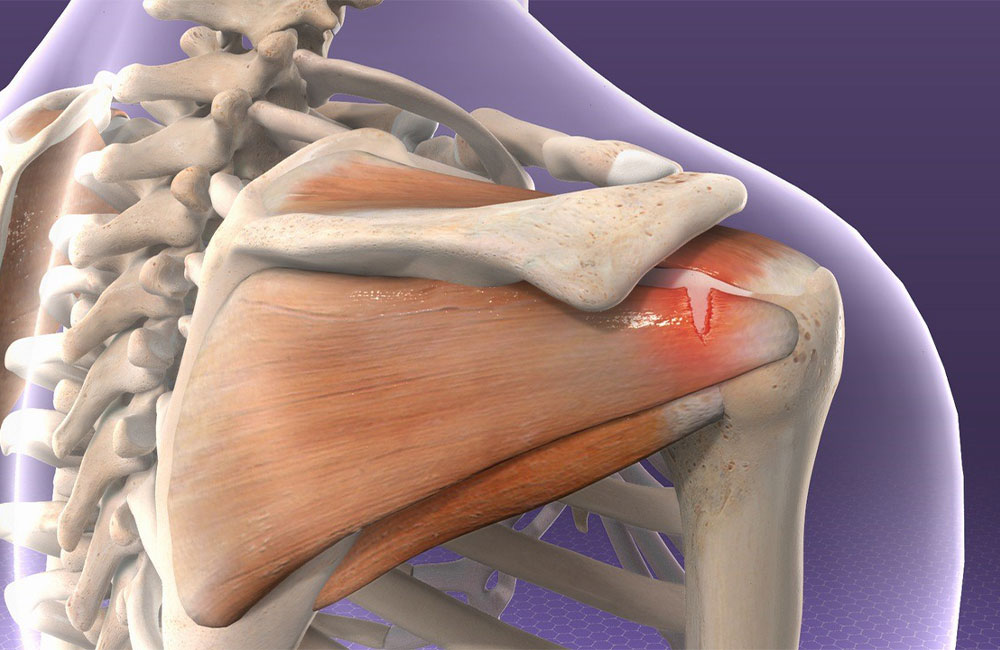
Frozen shoulder, medically known as “adhesive capsulitis,” is characterized by the thickening, stiffening, and formation of adhesions in the shoulder joint capsule, leading to restricted movement and pain. It can occur due to underlying trauma or systemic diseases such as diabetes, thyroid disorders, and heart conditions. In approximately half of the cases, no underlying cause is found. Patients typically experience increasing pain followed by shoulder joint movement limitations, making it challenging to perform daily tasks.
Frozen shoulder generally occurs in three stages:
1. Freezing Stage: Pain in the shoulder increases, and movement restrictions begin. This stage can last from a few weeks to a few months.
2. Frozen Stage: Pain diminishes, but shoulder movements are severely restricted. This stage can last for several months.
3. Thawing Stage: Shoulder movements gradually return. This stage can last from a few months to several years.
How Is Frozen Shoulder Diagnosed?
The diagnosis of frozen shoulder is primarily made through a doctor’s examination. If the range of motion in the shoulder joint does not improve even with passive manipulation, frozen shoulder may be suspected. To confirm the diagnosis and identify potential causes, X-rays, ultrasounds, and MRIs may be conducted. If no other issues are identified through imaging, treatment for frozen shoulder can begin.
How Is Frozen Shoulder Treated?
The first line of treatment typically involves conservative, non-surgical methods. The goal here is to manage pain, reduce inflammation, and increase shoulder mobility. The most important approaches include:
1. Physical Therapy and Exercises:
- Stretching Exercises: Special stretching exercises are performed to improve the flexibility of the shoulder capsule. These should be done carefully, considering the pain level.
- Mobilization Techniques: Physical therapists may use manual therapy techniques to mobilize the shoulder joint.
- Strengthening Exercises: Low-resistance exercises can be performed to strengthen the muscles around the shoulder.
2. Medication:
- Pain Relievers: Nonsteroidal anti-inflammatory drugs (NSAIDs) can be used to reduce pain and inflammation.
- Corticosteroid Injections: Corticosteroid injections into the shoulder joint can quickly reduce inflammation and pain, typically used alongside physical therapy.
- Heat and Cold Applications:
- Heat Therapy: Using warm compresses or heating pads can help relax shoulder muscles and reduce pain.
- Cold Therapy: Ice applications can reduce pain and swelling, especially during acute pain periods.
Additional physical therapy modalities may also be utilized at different stages of treatment.
Can Intra-Articular Injection Therapy Be Used for Frozen Shoulder?
Intra-articular injections can be beneficial, especially in the active phases of treatment. Steroid injections, in particular, can significantly reduce inflammation and swelling in the shoulder joint capsule, leading to decreased pain and improved participation in physical therapy. Typically, a noticeable reduction in pain is observed within a few days after the injection. If necessary, repeated injections may be administered several months apart. Caution is advised when administering steroid injections, especially in diabetic patients.
Another injection method is platelet-rich plasma (PRP) injections. More research is needed regarding PRP’s effectiveness, but some studies suggest it may help reduce inflammation and accelerate healing. PRP is typically considered for cases that do not respond to conservative treatment or for recurrent frozen shoulder cases.
Is Surgical Treatment Necessary for Frozen Shoulder?
Surgical intervention for frozen shoulder is generally considered when conservative methods (physical therapy, medication, injections) do not yield sufficient improvement. Surgery is preferred in cases where the patient continues to experience pain, has significantly restricted shoulder mobility, and where quality of life is severely affected.
Surgical criteria include:
1. Patients Who Do Not Respond to Conservative Treatments:
- Patients who do not achieve adequate improvement within 6-12 months despite receiving physical therapy, medication, and injections.
- Patients with long-lasting shoulder pain and stiffness (generally 1 year or more).
2. Severe Movement Restriction:
- Situations where shoulder mobility is severely limited, making it difficult to perform daily activities.
3. Severe and Persistent Pain:
- Patients who experience severe and disruptive pain, even at rest.
4. Conditions Resistant to Other Treatments:
- Cases where corticosteroid injections, PRP therapy, and other conservative methods are ineffective.
The first surgical option is manipulation of the shoulder joint under anesthesia. This involves passive movement of the shoulder joint to stretch the capsule and release adhesions. This method is used to provide sudden stretching of the capsule.
Another option is arthroscopic capsular release, a minimally invasive procedure where small incisions are made, and the capsule is cut and adhesions removed using arthroscopy. This method is preferred due to its shorter recovery time and lower complication risks.
In necessary cases, both arthroscopic techniques and manipulation can be performed together.
Post-surgery, physical therapy is crucial for regaining shoulder mobility and strengthening muscles. Pain management with pain relievers and other supportive treatments will be implemented after surgery. Regular check-ups with the doctor are important for monitoring the recovery process.
The decision for surgical intervention should be made by an orthopedic specialist, considering the patient’s overall health, age, lifestyle, and the potential risks of surgery. The patient’s expectations and goals also play a significant role in this decision.
In conclusion, frozen shoulder is a condition that significantly impacts daily life and diminishes quality of life. Patient compliance with treatment is crucial, and coordination among an orthopedic doctor, physical therapy doctor, and physiotherapists is essential for effective management.