What Is a Shoulder Dislocation?
A shoulder dislocation occurs when the humerus bone in the upper arm separates from the shoulder joint. This condition typically arises from trauma, falls, or sports injuries.
Patients may experience sudden and severe pain in the shoulder, along with deformity. Movement is restricted, and swelling and bruising may be observed in the shoulder area. The arm often hangs down and forward.
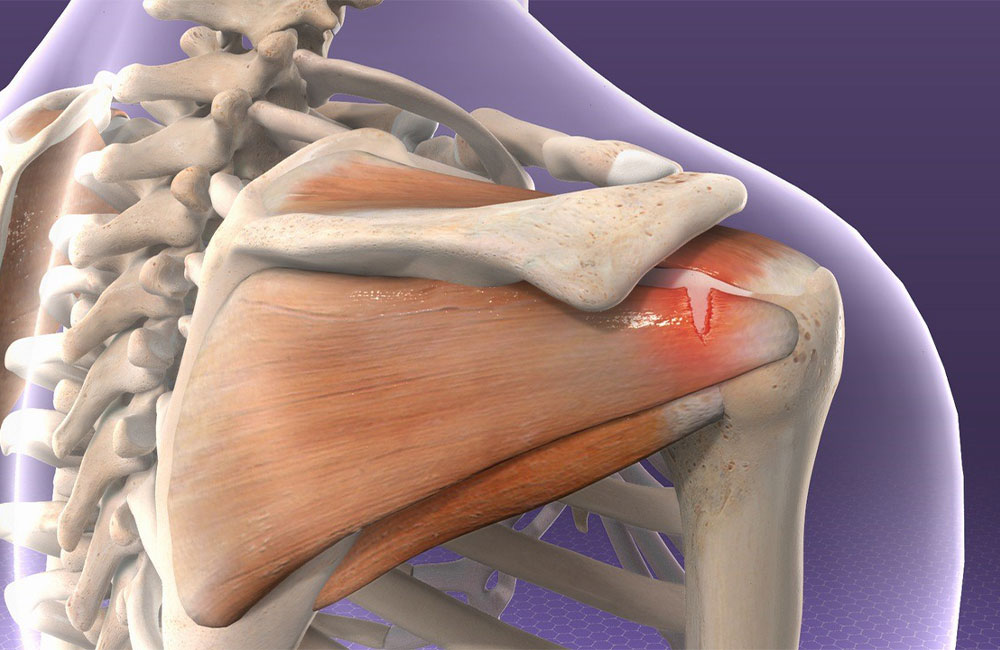
The shoulder joint is one of the most mobile joints in the body, and several key structures help maintain its stability:
- Capsule and Ligaments: Glenohumeral ligaments stabilize the shoulder joint, with the inferior glenohumeral ligament being one of the most important stabilizers.
- Labrum: The glenoid labrum deepens the socket of the shoulder joint, helping to hold the head of the humerus in place.
- Rotator Cuff Muscles: The supraspinatus, infraspinatus, teres minor, and subscapularis muscles stabilize the shoulder joint and enable movement.
- Biceps Tendon: The long head of the biceps tendon provides stability at the front of the shoulder.
- Dynamic Stabilizers: The periscapular muscles and other surrounding shoulder muscles provide dynamic stability.
Shoulder dislocations usually occur in either an anterior (front) or posterior (back) direction:
- Anterior Dislocation: This is the most common type of shoulder dislocation, often resulting from excessive abduction (side opening) and external rotation (outward turning) of the arm, causing the head of the humerus to move out from the front of the glenoid fossa.
- Posterior Dislocation: This is less common and typically occurs due to electric shocks, epileptic seizures, or direct trauma, causing the head of the humerus to move out from the back of the glenoid fossa.
Various structures may be damaged during a shoulder dislocation:
- Capsule and Ligaments: The shoulder joint capsule may tear or stretch, and the glenohumeral ligaments can be damaged.
- Labrum: Tears of the labrum, known as Bankart lesions, are associated with anterior dislocations.
- Rotator Cuff Muscles: Tears or tendinitis in the rotator cuff muscles may develop.
- Bone Structures: A fracture described as a Hill-Sachs lesion may occur on the head of the humerus opposite the direction of the dislocation, as well as fractures on the edge of the glenoid.
- Nerve and Vessel Structures: Axillary nerve injuries are common, as well as possible brachial plexus injuries. Damage to these nerves can lead to difficulty in moving the arm and shoulder, as well as loss of strength and sensation.
Shoulder dislocations typically result from traumatic events or specific movements. Particularly in chronic recurrent dislocations, certain movements can lead to the shoulder dislocating continuously. Initially starting with a traumatic event, if untreated, this process can result in recurring dislocations even during simple daily movements. Such movements may include:
- Excessive Abduction:
- Excessive lateral opening of the arm can place undue stress on the shoulder joint, leading to dislocation.
- External Rotation:
- During outward rotation of the arm, especially in sports activities (e.g., baseball pitching), the shoulder joint is at risk.
- Falling from a Height:
- Falling onto an outstretched hand or arm can place excessive load on the shoulder joint.
- Lifting Heavy Loads:
- Putting excessive stress on the shoulder joint can compromise its stability.
Aside from these movements, a family history of recurrent shoulder dislocations may indicate a genetic predisposition to weakness in connective tissues, increasing the risk for shoulder dislocation.
Similarly, individuals who have previously experienced a shoulder dislocation may have weakened or damaged ligaments and structures that hold the shoulder in place, making them candidates for recurrent dislocations.
Finally, individuals with hypermobility syndromes (such as Marfan, Ehlers-Danlos, or Down syndrome) are at greater risk for recurrent shoulder dislocations.
What Should I Do If I Experience My First Shoulder Dislocation?
A shoulder dislocation is very painful and should be treated by a healthcare professional. Failure to do so may result in more complex conditions.
First, do not move your shoulder and keep it in a stable position. Attempting to reset the dislocation can cause further damage.
Next, immobilize your arm close to your body with a simple sling. This will reduce pain and help prevent additional injuries.
If possible, apply a cold pack or ice gel. Seek medical attention at the nearest healthcare facility. After necessary evaluations and tests, a doctor will use sedation medications to relocate your shoulder. It will then be immobilized.
Following these steps, you should consult an orthopedic specialist for further assessment and treatment.
Do I Need Surgery for a Shoulder Dislocation?
The decision to undergo surgery after the first shoulder dislocation should consider the patient’s age, activity level, and personal preferences. It is important to carefully weigh the advantages and disadvantages of surgical versus conservative treatment options.
In particular, surgery significantly reduces the likelihood of recurrent dislocations after the first occurrence in younger and athletic patients. If the structures injured during the first dislocation are not repaired, there is a 50% to 90% chance of experiencing recurrent dislocations. Additionally, patients who undergo surgery after the first dislocation have a 30% reduced likelihood of needing further surgeries later on.
The younger the patient is at the time of their first dislocation, the greater the risk of recurrence.
In athletes, those who undergo surgery after a shoulder dislocation are more likely to return to sports compared to those who do not have surgery.
In older patients, it is important to remember that shoulder dislocations may be accompanied by large muscle tears, which may also require surgical intervention.