What Is Patellar Instability?
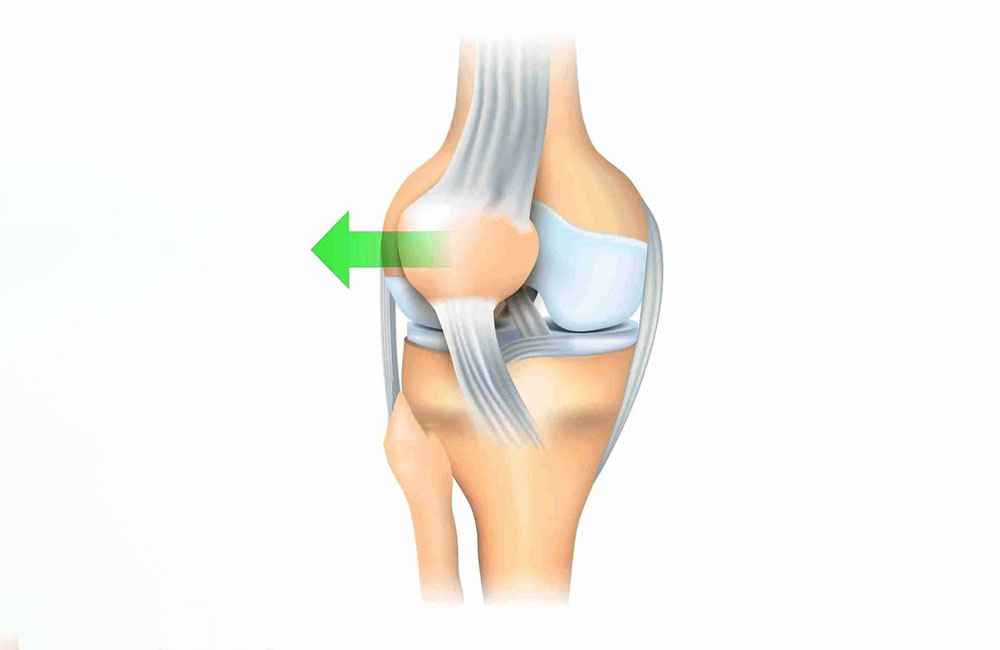
The Patella, or kneecap, is a bone at the front of the knee where our strongest muscles attach. The kneecap moves within a groove on the thigh bone (femur) during knee bending and straightening. Several ligaments and muscles work to keep the kneecap in place, and any disturbance in this harmony can lead to dislocation or instability of the kneecap.
It can generally be seen in two ways:
Complete Dislocation: This occurs when the kneecap completely displaces from its groove to the outer side of the knee. During this dislocation, the ligaments holding the kneecap may tear or get injured. Additionally, injuries or fractures can occur in the cartilage surface beneath the kneecap as it moves out of the groove.
Partial Dislocation: In this case, the kneecap has partially displaced outside the groove.
What Are the Symptoms of Patellofemoral Instability?
Patients often experience a dislocation of the kneecap after trauma, typically accompanied by swelling and limited movement after the kneecap returns to its position. During a test where the kneecap is gently pushed outward, patients may feel a fear of dislocation.
The kneecap can shift upwards and outwards during knee movements.
X-rays and MRI images of the knee are crucial for diagnosis and treatment planning. MRI can assess both the edema beneath the cartilage and the condition of the ligaments that keep the kneecap in place.
Who Is at Risk for Kneecap Dislocation?
The first dislocation typically occurs after trauma, often accompanied by an injury to the anterior cruciate ligament (ACL). Therefore, those engaged in contact sports (like soccer and basketball) are at a higher risk.
Beyond trauma, some individuals are structurally at risk:
- The groove for the kneecap may be shallow.
- Issues with connective tissue or hyperelasticity (e.g., Marfan syndrome, Ehlers-Danlos syndrome).
- The placement of the kneecap may be abnormally low or high.
- The femur may be rotated inward or the tibia outward.
- Improper leg alignment (such as knock-knees or bowlegs).
Instability may not always be accompanied by pain. In chronic cases, pain may be secondary; patients often report feeling unable to control their kneecap and experiencing weakness.
What Is the Treatment for Patellofemoral Instability?
In these cases, MRIs and, if necessary, CT scans taken after the first dislocation provide guidance for treatment. Sometimes, when the kneecap dislocates, a piece of cartilage may break off and become a free floating fragment within the joint. In such cases, a semi-urgent surgical plan is made to remove or repair this cartilage fragment while addressing the underlying causes. If there is no cartilage injury, treatment focuses on rehabilitation that strengthens the muscles around the knee.
Strengthening exercises typically begin two weeks after the dislocation and continue for 2-3 months. The average return to sports for an athlete is about 4-5 months.
The risk of recurrent dislocation is 20-40% after the first dislocation, increasing to over 50% after a second.
What Surgeries Are Performed for Recurrent Kneecap Dislocations?
If there are no underlying bony deformities following dislocations, the primary surgery is reconstruction of the ligament that keeps the kneecap in place (MPFL reconstruction). In this surgery, a tendon taken from the inner side of the knee is placed between the kneecap and the femur using special techniques. This helps prevent the kneecap from moving outward during knee movements.
If there is an issue with the height of the kneecap, adjustments are made to the tendon’s relationship with the femur.
In cases where the groove for the kneecap is too shallow, additional procedures to deepen this groove may be performed.
The rehabilitation period after surgery typically lasts about 6-9 months. In the first phase, exercises to improve knee range of motion are gradually increased. The second phase focuses on strengthening the muscles around the knee and balance training, while the third phase involves exercises to return to sports.
The results of the surgery are generally very positive. Patients can usually engage in daily and sporting activities comfortably within a year.
For more detailed information, you can visit my YouTube channel: @profdrhalukcabuk.